Yesterday I had difficulty breathing upon. waking up, and felt very dizzy and ill. I’ve had an annoying bit of a cough for weeks, especially when prone and I’d wake up coughing. Having already heard that some people with MS have a “neurological cough, I parked it as a wait and see concern.
My best peak expiratory flow is normally a decent 525. Yesterday it was down to 300, edging towards the Red Zone for me, where emergency treatment is called for. I have occasional asthma, most often triggered by infection, hence the peak flow meter. My Apple Watch detected SPO2 (blood oxygen levels) were dipping down to 86%, indeed during past week they were at 79% at one point. No wonder my brain could not function at all, and I hadn’t enough cognitive facility to even understand what was happening.
Some academic reading about MS infection & environmental triggers
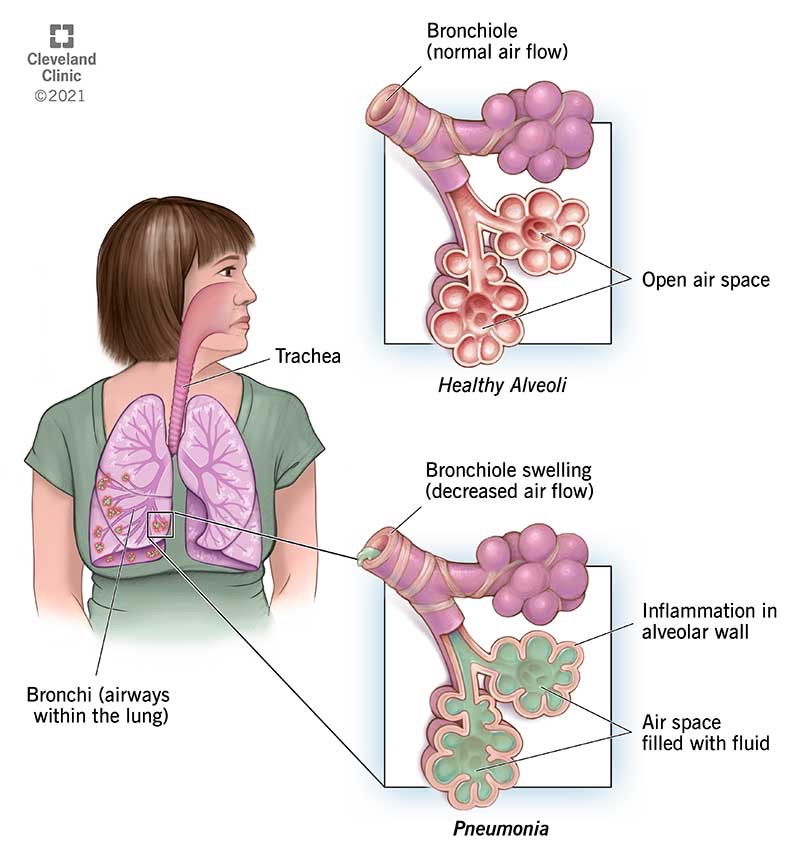
I emailed my GP, best way by far to contact the surgery, and explained all. As I was unable to leave the apartment he phoned me to discuss and said it was very obvious I have a bacterial aspiration pneumonia, originating from my poor cough reflex, weak breathing muscles, and inadequate swallowing function. I can’t always direct food and liquids properly into my stomach and when some does go down the wrong way my cough reflex doesn’t always detect or response inadequate. Food and liquid gathering in the lung naturally sets up a bacterial infection. When that infection starts to get serious it considerably worsens MS symptoms, apart from being potentially serious in itself.
The GP prescribed an antibiotic, as well as steroid to help open up the bronchioles. Prescription sent to pharmacy around corner. Certainly the steroid has kicked in nicely and my peak flow read as over 400 this morning. I’m still dizzy & weak all over, have bad postural tremor, but some of my cognitive abilities have improved. The pneumonia is still there as per SPO2 still dipping well below normal, not surprising as immune system has to surround infection with immune cells building up temporary debris as it starts to work. Also advised to double or even treble my routine Symbicort inhaler. The antibiotic will clear it within the week.

Aspiration pneumonia is the most common cause of death most directly caused by MS, so we are talking about a pretty serious type of event to be happening here. The most common cause of death overall in MS is secondary to being unable to exercise, and that is cardiovascular, mainly affecting heart; as in other autoimmune conditions also probably related to inflammatory processes.
Some academic reading re lung complications being frequent terminal event in advanced MS
I will have to regularly keep a check on peak flow and SP02, maybe twice weekly, to keep an eye on the pattern. The idea being to get an antibiotic before the worst starts to happen. I have ordered a spirometer to help keep an eye on my inspiration depth, and it is used as an incentive to train chest muscles into achieving the best they can.
Lung complications as terminal event in MS
A less serious but quite upsetting angle is that during my sleep especially, I am losing most bladder control, I mean I am “wetting the bed”. Fine in my own house, but not so in hotel guest rooms. Have to bring even more stuff in my luggage. “Why do you bring such a large luggage case”. People invariably probe me on that, and get all embarrassed when I reveal about the stoma supplies after starting with the dead body account. After a few coughs, splutters, and a hiatus of embarrassed silence, the conversation invariably turns into “aren’t you just great to be travelling the way you are, you are amazing”.
If you have MS and there’s a sharp deterioration
Look out for infection. More commonly in lung, sinuses, bladder or dental. You might not even have a fever in spite of a serious infection.
Dental: check gums for any small abscesses (dead teeth don’t hurt), and check tonsils whilst you are at it. Some nasty tonsillitis doesn’t hurt either. Checking for swollen, sometimes sore lymph nodes in the neck can be the first clue.
Bladder: If bladder doesn’t empty properly, residual urine can easily grow bacteria, and this infection can be relatively silent, especially when you already have neurogenic bladder dysfunction. You can buy urine testing sticks online or in pharmacy, and some of these can test for other things going on too. But to check for likely urinary infection you want one that includes checks for leukocytes, blood, protein. If you are prone to bladder retention you could do a routine weekly check.
Sinuses: you will get a headache in the cheeks and between the brows, and to sides of nose, all made worst by stooping. Very common with of after any respiratory virus, and some people are more prone than others. If like me, you have a badly deviated septum a surgery can help address this, and sinus rinses can sometimes help. Sinus infections can be associated with lung infections too.
Lung: Can be viral, (the “it’s going around” type) where supportive symptomatic care like resting is the only thing to do unless it gets worse. Good to check the SPO2 when you get a chest infection, and a simple finger gadget can be bought online or purchased in a pharmacy. A secondary bacterial infection can set in after a week or so. A viral cough can last seemingly forever, so that alone is not a sign, keep an eye on temperature and SPO2 and increasing sputum. Bacterial infections don’t always produce much sputum at all, as the material can be “stuck” deep in the lungs, and can be relatively clear too. When there is brown or purple sputum (older blood from alveoli) that is a pretty sure sign of bacterial pneumonia whatever else symptoms present or otherwise. Smallish amounts of brighter red sputum alone is likely to be from bronchial inflammation, but needs to be addressed via the doctor. An antibiotic and possibly a steroid will be prescribed by your doctor.
Always best to keep away from the hospital emergency departments where possible, but there are signs that should lead you there without hesitancy when they occur. I was borderline there, as I had lost so much mobility and was on the point of not being able to look after myself at all, especially living alone as I do. But I hate public hospitals with a vengeance and have a changeable relationship with private ones.
The older you are, the earlier the red flags occur. If you can still get on your feet without undue added impairment, your temperature isn’t up too much, you are not coughing blood, your SPO2 is mostly keeping over 93, broadly speaking your local doctor can treat you. If you are running down into 80s SPO2 and are younger it’s still possible the GP might address it. If there are any signs of SEPSIS, dial emergency services immediately and don’t forget to try and ask “could this be sepsis?” When you reach the hospital. On any case your GP should be in the best position to advise, and like my own one said “get back to us immediately if things get worse, or haven’t improved much after end of antibiotics.
Suggested Devices to assist in your own self-assessment
Urine Infection Testing Kit There are many on the market, I’ve added the link to one just to let you see a typical one. Google for the best value, and especially if you have to repeat the test frequently you need to get value for money.
Pulse Oximeter to measure SPO2, blood oxygen. This is just one source. Again Google for best value and ratings. Keep a spare battery for your model.
Peak Flow Meter to measure power of expiration, it assesses if there is narrowing of the tubes from your lungs.
Spirometer A typical example for incentive use to help build up your deep breathing power. Others are neat with digital read outs, some can be connected to internet. Shop around.
High quality precision digital thermometer This is an example of a non-contact one. Check over the internet for various such models. Make sure you keep a spare battery for your chosen model.
Consider a Smart Watch It is useful for any person with MS to wear a smart watch. The things for you to look out for is primarily an alert system for fall detection and to send alarm notifications to relatives, neighbours, even emergency service. Secondary useful functions would be health monitoring. SPO2 can be tracked, heart rate, heart arrhythmia, wrist temperature, mobility, fitness. These functions aren’t always as reliable as using standalone gadgets, although some of the latter can be connected to your phone/internet.
I personally have an Apple Watch, which provides a useful view of longer term trends and has tracked the overall deterioration in my mobility. I find it more useful to monitor longer term trends than day to day stuff. Above all I have it for fall detection and automatically notifying relatives. It can alert them, and if I am unable to answer their call to me to check things aren’t too bad, they can put the plan in action to check in on me.
All the data I can provide to the GP, especially over a phone consultation when I cannot attend the surgery, is extremely helpful in assisting the doctor in making the decision to prescribe or refer to an emergency department.
